
Category: Accidents and Incidents
Fuel Switches in the Cutoff Position on China Eastern flight 5735
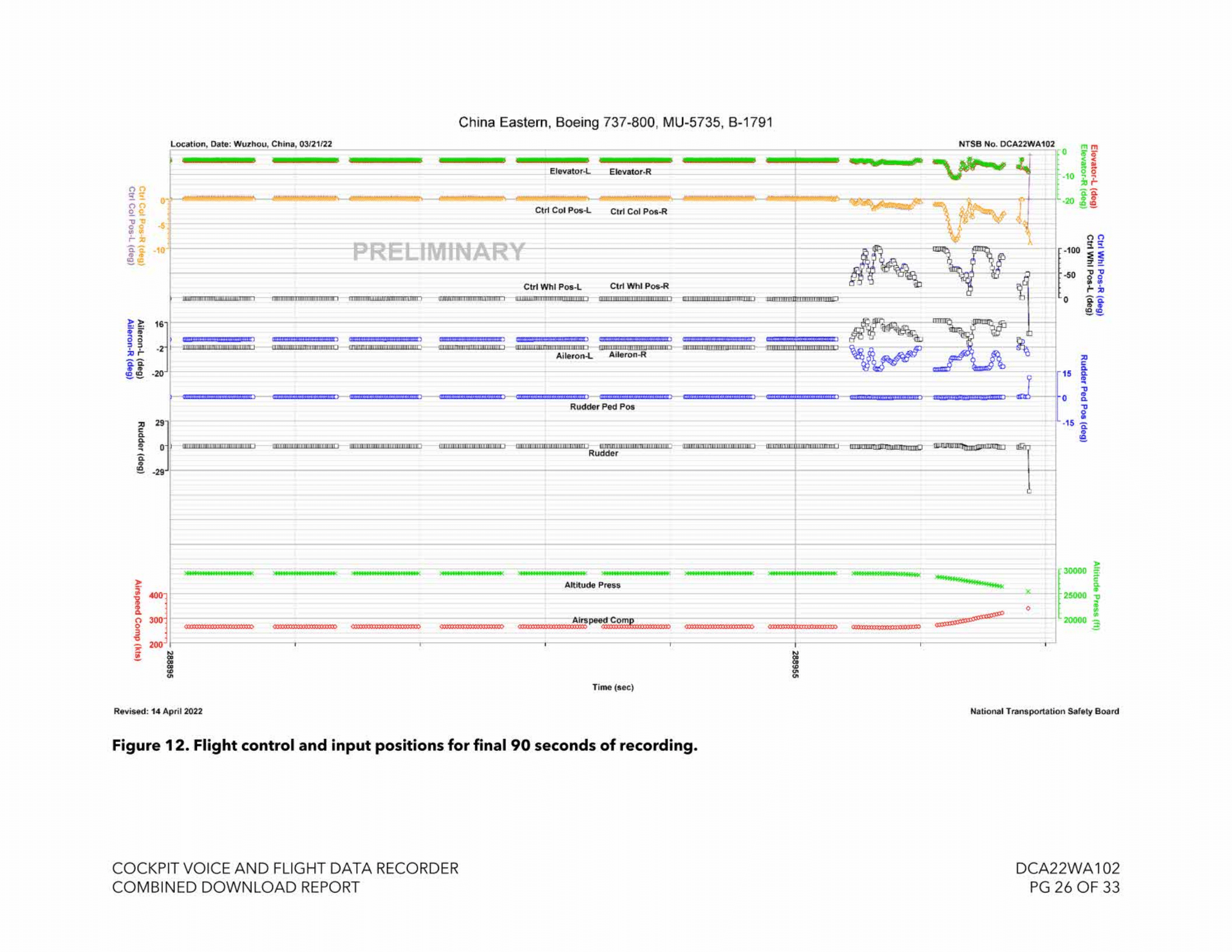
On the 21st of March 2022, a Boeing 737 passenger airliner crashed into a mountain. This was China Eastern Airlines flight 5735 flying from Kunming to Guangzhou in the People’s Republic of China. All 132 souls on board perished in the crash. This was the first fatal crash of a Chinese mainline carrier in nearly twelve years.…
Read more… 8 May 26
Ferry Tank Failure: Successful SR22 Ditching in the Pacific

In 2015, I shared a video of an SR22 whose pilot successfully deployed his Cirrus Airframe Parachute System (CAPS) off of the coast of Maui, Hawai’i. I wrote at the time that I would update once the final report came out. I am rather behind on my todo list, I’m afraid. The Cirrus SR22 is at…
Read more… 24 Apr 26
A Preventable Collision on Runway 4

On the 22nd of March 2026, a landing jet struck a fire truck that a controller had cleared onto the active runway at LaGuardia Airport in New York, the first fatal accident at LaGuardia in 34 years. Somewhat bizarrely, the previous accident, when USAir flight 405 crashed on take-off after ice buildup on the wings, occurred…
Read more… 27 Mar 26
The Man in the Right Seat at Prestwick
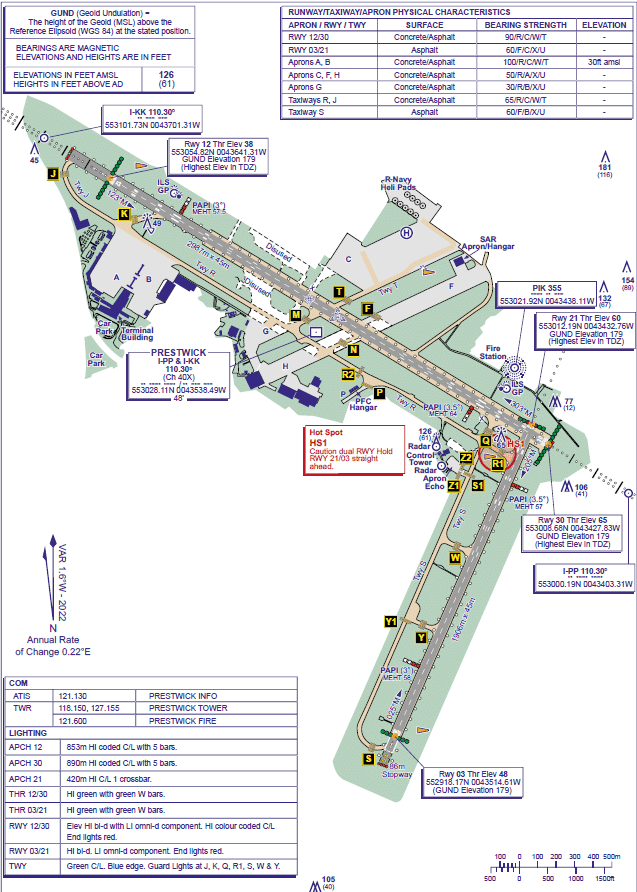
On the 23rd of April 2024, a Piper Archer II crashed in South Ayrshire, Scotland, after losing power. There were two on board. Both suffered serious injuries and the light aircraft, a 48-year old PA-28 registered in the UK as G-BVNS, will never fly again. The AAIB report makes a clear case for carburettor icing…
Read more… 20 Mar 26
Hot Air Balloon Rescue in Texas

On the morning of Saturday the 28th of February 2026, a brightly coloured hot air balloon launched near Longview, Texas. There were two onboard. I’ve not seen anything that mentions the weather. It would be very interesting to know more about what the wind was that morning. So far, the only data I’ve seen is…
Read more… 6 Mar 26
TNflygirl and the Beech Debonair
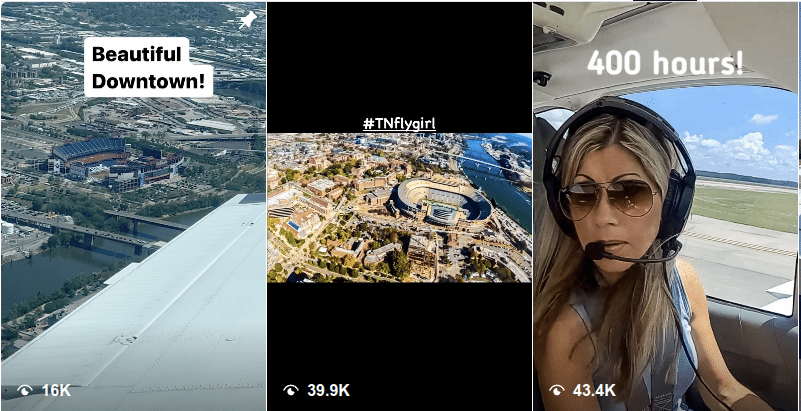
On the 7th of December 2023, a Beech 35-C33 Debonair crashed into terrain. The private pilot and the passenger, the pilot’s father, were both killed on impact. The private flight departed Knoxville Downtown Island Airport for a 430-nautical-mile flight to Saline County Regional Airport in Arkansas to pick up some avionics equipment. It was a…
Read more… 20 Feb 26
Accident Reports
 At All Costs
At All Costs
On the 11th of December 2024, the passenger in the right seat of a 1973 Grumman AA-5 was recording a video as they approached Pearland Regional Airport in Texas. The…
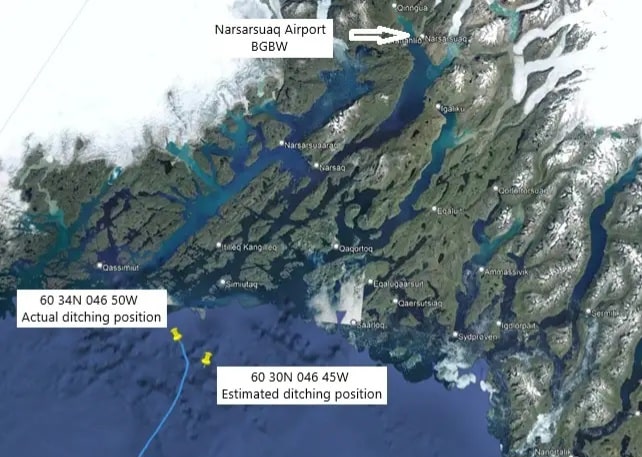 Any Landing You Can Float Away From: Successful Ditching in the Arctic
Any Landing You Can Float Away From: Successful Ditching in the Arctic
On the 29th of July 2024, a light aircraft encountered engine trouble off the coast of Greenland and was forced to ditch in the North Atlantic. The aircraft was a…
Demystifying
 The Pilots, the Probes, and the AF447 Verdict
The Pilots, the Probes, and the AF447 Verdict
On the 21st of May 2026, the Paris Court of Appeal convicted Airbus and Air France of involuntary manslaughter for their roles in the crash of Air France flight 447,…
 Meowing on Guard (an attempt at an explanation)
Meowing on Guard (an attempt at an explanation)
Last week a video went viral and it’s been fun to see the mainstream media coverage try to cover two pilots who were heard making animal noises on the radio. …
History
 The First Jet to Land on an Aircraft Carrier (Deliberately)
The First Jet to Land on an Aircraft Carrier (Deliberately)
“The Vampire was the first jet to land on a moving aircraft carrier deliberately.” This quote from Airshow Luke, our MC at the Legacy of Liberty airshow, made me almost…
 Four Point Two Stars Where You Only Stop If You Have To
Four Point Two Stars Where You Only Stop If You Have To
I always look up airports when I’m writing about them, partly out of habit and partly because I’m afraid I’ll miss an important detail. When I was writing Any Landing…
Fun Stuff
 Aviation Stories You Might Have Missed
Aviation Stories You Might Have Missed
I hope you all are having a wonderful holiday season. This week, I’ve put together a compilation of interesting items in the press that you might have missed while enjoying…
 Nathan Pyle Strange Worlds
Nathan Pyle Strange Worlds
Thank you so much for all the kind words. I don’t quite have the wherewithal to respond to each of you individually but I very much appreciate all of you…






